 Understanding Esophageal Dysmotility: Symptoms, Causes, and Treatments
Understanding Esophageal Dysmotility: Symptoms, Causes, and Treatments
Esophageal dysmotility disrupts the normal movement of food and liquids through the esophagus, causing symptoms like difficulty swallowing and chest pain. This article explains what esophageal dysmotility is, its causes, symptoms, and treatment options to help you manage this condition.
Key Takeaways
•Esophageal dysmotility is characterized by impaired movement of food and liquids, with common symptoms including dysphagia, chest pain, and heartburn.
•Motility disorders can be classified as primary, such as achalasia and diffuse esophageal spasm, or secondary, like scleroderma, each requiring tailored treatment approaches.
•Effective management of esophageal dysmotility includes lifestyle modifications, medical therapies, and potential surgical interventions, aimed at alleviating symptoms and preventing complications.
What is Esophageal Dysmotility?
Esophageal dysmotility refers to a range of disorders that impair the normal movement of food and liquids through the esophagus. These disruptions can lead to significant discomfort and challenges in everyday life. Common symptoms include chest pain, difficulty swallowing (dysphagia), esophageal dysfunction, and heartburn, making it a formidable condition to manage.
Esophageal motility disorders are divided into primary esophageal motility disorders and secondary esophageal motility disorders. Primary disorders mainly affect the esophagus itself, such as achalasia, where the lower esophageal sphincter (LES) fails to relax, preventing food passage. Secondary disorders, like scleroderma, can impact the entire body but also affect esophageal function. Precise terminology, such as 'dis esophagus,' is essential in the diagnostic classification and differentiation of esophageal motility abnormalities, including conditions like achalasia and esophageal spasms.
Anatomy of the Esophagus
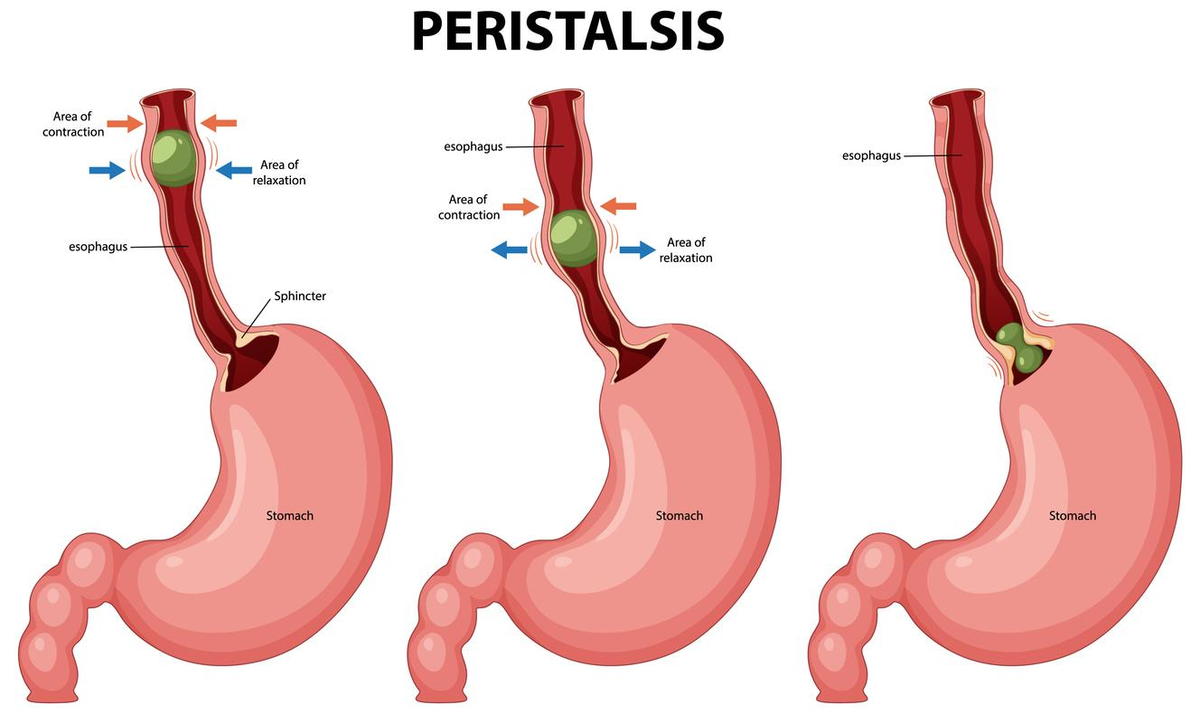
The esophagus is a muscular tube, approximately 25 to 33 centimeters in length in adults, that conveys food and liquids from the throat to the stomach. This journey is facilitated by two critical structures: the upper esophageal sphincter (UES) and the lower esophageal sphincter muscle (LES). The UES, composed of striated muscle, opens to allow food entry. In contrast, the LES, a smooth muscle, prevents stomach contents from refluxing back into the esophageal body. The coordinated action of the esophagus muscles aids in this process.
Peristalsis, the wave-like muscular contractions, plays a vital role in moving food down the esophagus. This process involves a coordinated contraction of the esophageal muscles and esophageal peristalsis, ensuring that food reaches the stomach efficiently, alongside normal peristalsis. The esophagus itself is divided into a proximal portion with striated muscles and a distal portion with smooth muscles, each contributing to its overall function.
Diagnostic imaging and endoscopic evaluation often focus on the esophageal lumen to identify abnormalities such as dilation, food stasis, or mucosal changes, which are essential for the assessment of esophageal motility disorders.
Understanding the esophagus's anatomy is crucial for grasping how esophageal motility disorders disrupt normal digestion. When these muscles and sphincters fail to work correctly, it leads to the various symptoms and complications associated with esophageal dysmotility.
Pathophysiology and Disease Mechanisms
Esophageal motility disorders arise when the normal, coordinated movement of the esophagus is disrupted, leading to a range of symptoms such as dysphagia, chest pain, and regurgitation. At the core of these motility disorders is a breakdown in the precise coordination between the upper esophageal sphincter (UES), the lower esophageal sphincter (LES), and the esophageal body. In healthy individuals, these structures work together to propel food smoothly from the mouth to the stomach. However, in primary esophageal motility disorders like achalasia, the lower esophageal sphincter fails to relax properly, causing food to accumulate and resulting in esophageal dilation and impaired swallowing.
Secondary esophageal motility disorders, such as those caused by systemic diseases like scleroderma, involve progressive fibrosis and atrophy of the esophageal muscles. This leads to weakened or absent esophageal contractions, making it difficult for the esophagus to move food efficiently. Esophageal spasm, including diffuse esophageal spasm, is another type of motility disorder characterized by uncoordinated and sometimes forceful esophageal contractions. These spasms can trigger intense chest pain and difficulty swallowing, further complicating normal digestion.
Understanding the underlying pathophysiology of esophageal motility disorders—whether due to malfunctioning sphincters, abnormal esophageal contractions, or muscle atrophy—is essential for developing targeted treatment strategies and improving patient outcomes.
Epidemiology and Impact
Esophageal motility disorders are more common than many realize, affecting up to 10% of the population at some point in their lives. The likelihood of developing esophageal dysmotility increases with age, with most cases occurring in individuals over 50. These motility disorders can significantly disrupt daily life, as symptoms like dysphagia and chest pain often interfere with eating, socializing, and overall well-being.
Beyond the immediate discomfort, esophageal motility disorders can lead to serious complications. Individuals with these conditions are at increased risk for gastroesophageal reflux disease (GERD), esophagitis, and even esophageal cancer. The persistent symptoms of esophageal dysmotility, such as dysphagia and chest pain, can also contribute to anxiety and reduced quality of life.
The economic impact is substantial, with annual healthcare costs related to esophageal motility disorders exceeding $10 billion in the United States alone. This underscores the importance of early diagnosis, effective management, and ongoing research to reduce the burden of these conditions on both individuals and society.
Symptoms of Esophageal Dysmotility
Living with esophageal dysmotility often means grappling with a range of challenging symptoms. Dysphagia, or difficulty swallowing, is a primary symptom, making it hard to eat and drink normally. This can result in food becoming trapped in the esophagus, causing significant discomfort. Esophageal dysmotility can also present with a variety of gastrointestinal symptoms, such as chest pain and dysphagia, which are essential for clinical evaluation.
Chest pain, particularly after eating, is another common complaint, often mistaken for heart issues. Dysphagia and chest pain, along with regurgitation, where food comes back up without forceful vomiting, are also prevalent. This symptom, along with heartburn and the sensation of food sticking in the esophagus, can severely impact one's quality of life due to stomach acid.
These symptoms not only disrupt daily activities but can also lead to anxiety and stress, further exacerbating the condition. In some cases, nasopharyngeal regurgitation may occur, indicating oropharyngeal dysfunction and helping to distinguish between oropharyngeal and esophageal causes of dysphagia.
Common Types of Esophageal Motility Disorders
Esophageal motility disorders encompass a variety of conditions that impede the normal movement of food through the esophagus, including primary motility disorders, other motility disorders, spastic esophageal motility disorders such as nutcracker esophagus and esophageal hypercontractility, and esophageal motility disorder symptoms. Each type has distinct characteristics and symptoms, ranging from achalasia to diffuse esophageal spasm, nutcracker esophagus, esophageal hypercontractility, and scleroderma esophagus, as well as other esophageal disorders, including functional esophageal disorders.
Manometric abnormalities are often observed in these disorders and are key to their diagnosis.
Understanding these types helps in identifying the specific challenges and treatment approaches for each disorder.
Achalasia
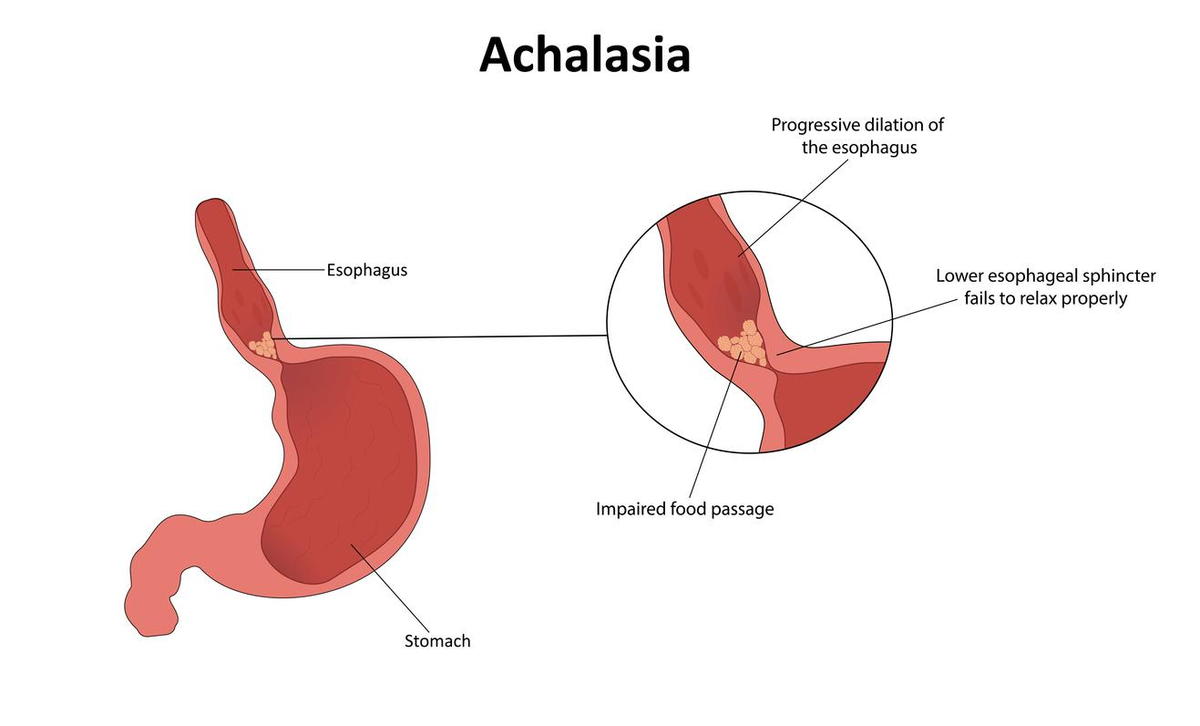 Achalasia is a rare and progressive disease characterized by the inability of the lower esophageal sphincter (LES) to relax properly during swallowing. This leads to a sensation of food being stuck and can cause significant stasis of food within the esophagus. Pathologically, achalasia is marked by a reduction in ganglion cells in the LES, surrounded by inflammatory cells.
Achalasia is a rare and progressive disease characterized by the inability of the lower esophageal sphincter (LES) to relax properly during swallowing. This leads to a sensation of food being stuck and can cause significant stasis of food within the esophagus. Pathologically, achalasia is marked by a reduction in ganglion cells in the LES, surrounded by inflammatory cells.
A distinct feature seen in diagnostic tests is the 'bird beak' appearance on an esophagogram, where esophageal dilation is observed with a narrow LES. Patients with oesophageal achalasia are at a higher risk of developing squamous cell carcinoma of the esophagus, especially after about ten years post-diagnosis. Additionally, some patients may have concurrent hiatal hernia, further complicating their condition.
Diffuse Esophageal Spasm
Diffuse esophageal spasm involves uncoordinated, often painful esophageal contractions of the esophagus, leading to significant disruptions in normal swallowing. Patients frequently experience chest pain and dysphagia as a result. These uncoordinated contractions can cause food to back up in the esophagus, making eating a distressing experience.
The hallmark of diffuse esophageal spasm is its unpredictable and erratic contractions, which can be severe and debilitating. Understanding this condition helps in distinguishing it from other esophageal motility disorders and tailoring appropriate treatment strategies.
Scleroderma Esophagus
Scleroderma esophagus is a secondary esophageal motility disorder associated with the autoimmune disease esophageal scleroderma. This condition leads to progressive fibrosis and thickening of the esophageal tissue, resulting in symptoms like gastroesophageal reflux disease, reflux disease, and reflux esophagitis. Scar tissue replaces the smooth muscle in the esophagus. This change results in a loss of peristalsis and a weakening of the lower esophageal sphincter (LES).
Diagnostic findings often show a dilated esophagus with weak or absent peristalsis and significant reflux. While motility is preserved in the proximal esophagus striated muscle portion of the esophagus, the overall function is severely compromised, making it challenging for patients to swallow effectively due to ineffective esophageal motility in the distal esophagus.
Causes of Esophageal Dysmotility
The causes of esophageal dysmotility are varied and can be classified into primary and secondary origins:
Primary causes include:
•Idiopathic factors
•Postviral infections
•Environmental influences
•Genetic predispositions
Secondary causes often involve systemic conditions that affect the entire body, such as autoimmune disorders like systemic sclerosis, which result in smooth muscle atrophy.
Chagas disease is a notable example of a secondary disorder that leads to esophageal dysmotility due to chronic mucosal irritation from chronic Infection. Other conditions, such as eosinophilic esophagitis, can cause narrowing of the esophagus, complicating the passage of food.
Additionally, congenital conditions such as esophageal atresia can result in esophageal dysmotility. Esophageal atresia is a congenital disability that often requires prompt surgical intervention to restore normal esophageal function and enable proper feeding and may necessitate subsequent surgeries.
Understanding these causes is crucial for accurate diagnosis and effective treatment.
Diagnosing Esophageal Dysmotility
Diagnosing esophageal dysmotility involves a combination of clinical evaluation and diagnostic tests. Accurately identifying the specific motility disorder helps in tailoring the most effective treatment plan.
Clinical Evaluation
The initial step in diagnosing esophageal motility disorders involves a thorough physical examination and a detailed patient history assessment. Understanding the patient's symptoms, medical history, and lifestyle can provide critical clues to the underlying motility disorder. Ruling out other potential causes of the symptoms ensures accurate diagnosis.
Evaluating the entire length of the esophagus is crucial, especially when differentiating types of dysphagia. Difficulty with both solids and liquids during swallowing typically suggests a motor disorder, necessitating further diagnostic tests to confirm the diagnosis.
Diagnostic Tests
Esophageal diagnostic tools include:
•Esophageal manometry: measures the coordination and strength of muscle contractions in the esophagus.
•High-resolution manometry (HRM): provides detailed insights into esophageal pressure patterns and peristalsis, invaluable for diagnosing esophageal motility disorders.
•Barium swallow studies: visualize esophageal movement and identify structural issues.
Endoscopy allows for direct visualization of the esophagus, helping to rule out physical obstructions like tumors. This procedure, combined with manometric and barium swallow studies, provides a comprehensive assessment of esophageal function and structure, facilitating accurate diagnosis.
Treatment Options for Esophageal Dysmotility
Various treatment options are available for managing esophageal dysmotility, ranging from lifestyle modifications to primary surgical management and medical and surgical interventions.
The choice of treatment depends on the severity of the symptoms and the specific type of motility disorder.
Lifestyle Modifications
Lifestyle modifications can significantly alleviate symptoms associated with esophageal dysmotility. These include:
•Eating smaller, more frequent meals reduces the workload on the esophagus and makes swallowing easier.
•Consuming softer foods to minimize the effort required from the esophageal muscles.
•Avoiding trigger foods.
•Practicing careful eating habits to enhance comfort.
Incorporating stress management techniques can be beneficial, as stress may exacerbate dysmotility symptoms. Simple changes like sitting upright while eating and avoiding late-night meals can also help manage the condition more effectively, making daily life more manageable.
Medical Therapies
Pharmacological interventions play a crucial role in managing esophageal motility disorders. Medications like nitrates and nifedipine help control symptoms by relaxing the esophageal muscles. Calcium channel blockers are commonly prescribed to manage the condition, providing relief from symptoms like chest pain and dysphagia.
Botulinum toxin injections are another effective treatment option, offering relief by relaxing the smooth muscle of the esophagus. These injections can provide symptom relief for up to a year, making them a valuable option for chronic management.
Surgical Interventions
Surgical interventions may be necessary for severe cases of esophageal dysmotility when other treatments have failed. Heller myotomy is a surgical technique that involves cutting the muscles of the esophageal sphincter to alleviate symptoms. This procedure can significantly improve the passage of food through the esophagus.
Peroral endoscopic myotomy (POEM) is a minimally invasive surgery used to treat esophageal motility disorders. Surgical dilation may also be performed to stretch the esophagus and alleviate narrowing. These interventions provide long-term relief and are often considered when medical therapies are insufficient.
Managing Chronic Esophageal Dysmotility
Managing chronic esophageal dysmotility requires ongoing care and regular follow-up appointments to monitor symptoms and adjust treatment plans. Keeping a symptom diary can help track changes in the condition and identify potential triggers, allowing for more personalized and effective management.
Patients are encouraged to work closely with their healthcare providers to ensure that their medical therapy remains effective. Regular monitoring and adjustments can help manage the condition more effectively, improving the patient's quality of life through chronic treatment.
Potential Complications
Untreated esophageal motility disorders can lead to severe health issues such as malnutrition and aspiration pneumonia. Difficulty swallowing and reduced food intake can result in significant nutritional deficiencies, impacting overall health.
Oropharyngeal dysphagia can lead to life-threatening outcomes like choking and pneumonia. Additionally, patients with achalasia have an elevated risk of developing esophageal cancer approximately ten years post-diagnosis, highlighting the importance of early and effective treatment.
Current Research and Future Directions
Research into esophageal motility disorders is rapidly advancing, offering hope for improved diagnosis and treatment. Innovations in high-resolution manometry and impedance monitoring have greatly enhanced the ability to accurately diagnose motility disorders, allowing for more precise identification of abnormal esophageal contractions and sphincter function.
On the treatment front, new procedures such as per-oral endoscopic myotomy (POEM) and botulinum toxin injections are expanding the options available for patients with challenging motility disorders. These minimally invasive therapies can provide significant symptom relief, especially for those who do not respond to traditional treatments.
In addition to medical and surgical advances, there is growing interest in the role of cognitive behavior therapy and other non-pharmacological interventions for managing symptoms and improving quality of life. Future research is focused on developing personalized treatment plans tailored to each patient's unique needs, as well as uncovering the genetic and environmental factors that contribute to esophageal motility disorders. As our understanding deepens, new preventive strategies and innovative therapies are likely to emerge, offering better outcomes for those affected by these complex conditions.
Living with Esophageal Dysmotility
Living with esophageal dysmotility involves making several adjustments to daily routines and habits to manage symptoms effectively. Incorporating peppermint into the diet can help relax the esophageal muscles, providing relief from spasms. Keeping a food diary is also beneficial, as it helps identify which foods trigger symptoms, allowing for better dietary choices.
Consulting a dietitian can provide personalized dietary advice and nutritional support, ensuring that nutritional needs are met despite the challenges of dysphagia. Stress management techniques, such as relaxation exercises, can also play a crucial role in alleviating symptoms, as stress often exacerbates esophageal dysmotility.
Support groups offer a platform for sharing experiences and strategies for managing the condition. Additionally, using extra pillows to elevate the head during sleep can help reduce nighttime significant acid reflux, further improving overall comfort and quality of life.
Summary
Understanding esophageal dysmotility is key to managing its impact on daily life. From recognizing symptoms and understanding the anatomy of the esophagus to exploring various treatment options, this guide provides a comprehensive overview of the condition. Lifestyle modifications, medical therapies, and surgical interventions all play roles in managing symptoms and improving quality of life.
Living with esophageal dysmotility requires ongoing care and adjustments. However, with the right strategies and support, it is possible to lead a fulfilling life. By staying informed and proactive, individuals can better navigate the challenges of this condition and maintain their well-being.